The retina is the tissue that contains the photoreceptors (the rods and cones) in the back of the eye. The retina is the part of the eye that turns light entering the eye into a signal that can be transmitted to the brain via the optic nerve. There are numerous conditions of the retina that can be diagnosed with a proper dilated eye examination. Some of the more common conditions are listed below.

For information on some of the other more common retinal conditions and their treatment, Dr. Thayer highly recommends a visit to the website of our superb local Retina specialty group, the New England Retina Consultants, at this link.
Macular Degeneration
a closer look

Normal Retina
Optic Nerve Head (ONH)

Early Stage-AMD
Yellow extracellular drusen deposits

Late Stage-AMD
*Background Darkening
overview
Age-related macular degeneration (AMD) is a disease associated with aging that gradually destroys the macula, a cluster of light-sensitive cells in the central part of the retina. The macula provides crisp central vision and allows you to see fine detail. Central vision is needed for seeing objects clearly and for daily tasks such as reading and driving.
AMD occurs in two forms, wet and dry.
Age-related macular degeneration develops gradually at first, but can progress abruptly to an advanced stage that requires immediate consultation with a vision care provider. Even though AMD causes no pain, it can lead to a loss of vision in both eyes. AMD is the leading cause of vision loss in Americans over 60-years-old.
Factors that may increase your risk of macular degeneration include:
- Age. This disease is most common in people over 60.
- Family history and genetics.
- Race. Macular degeneration is more common in Caucasians.
- Smoking. Smoking cigarettes or being regularly exposed to smoke significantly increases your risk of macular degeneration.
- Obesity. Research indicates that being obese may increase your chance that early or intermediate macular degeneration will progress to the more severe form of the disease.
- Cardiovascular disease. If you have had diseases that affected your heart and blood vessels, you may be at higher risk of macular degeneration.
Dry macular degeneration symptoms usually develop gradually and without pain. They may include:
- Visual distortions, such as straight lines seeming bent
- Reduced central vision in one or both eyes
- The need for brighter light when reading or doing close-up work
- Increased difficulty adapting to low light levels, such as when entering a dimly lit space
- Increased blurriness of printed words
- Decreased intensity or brightness of colors
- Difficulty recognizing faces
- A well-defined blurry spot or blind spot in your field of vision
Wet macular degeneration symptoms are essentially the same, but their onset can be much more sudden and severe.
It’s important to have routine eye exams to identify early signs of macular degeneration. The following measures may help reduce your risk of developing dry macular degeneration:
- Manage your other medical conditions. For example, if you have cardiovascular disease or high blood pressure, take your medication and follow your doctor’s instructions for controlling the condition.
- Don’t smoke.
- Maintain a healthy weight and exercise regularly. If you need to lose weight, reduce the number of calories you eat and increase the amount of exercise you get each day.
- Choose a diet rich in fruits and vegetables. Choose a healthy diet that’s full of a variety of fruits and vegetables. These foods contain antioxidant vitamins that reduce your risk of developing macular degeneration.
- Include fish in your diet. Omega-3 fatty acids, which are found in fish, may reduce the risk of macular degeneration. Nuts, such as walnuts, also contain omega-3 fatty acids.
- Take AREDS II Vitamins. The Age Related Eye Disease Study (AREDS) found that the formulation in AREDS II vitamins can slow or prevent the progression of dry macular degeneration.
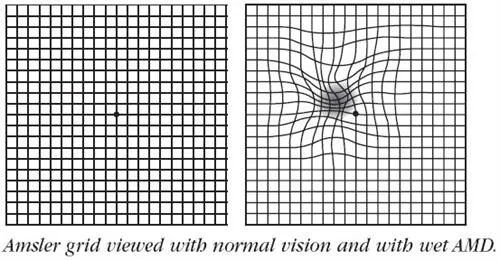 Amsler Grid Testing: The Amsler grid is a very simple test that can be done at home to detect worsening of macular degeneration. Using your reading glasses, you simply cover an eye and look at the center of the grid square, looking for any areas of distortion. You then repeat the test for the other eye.
Amsler Grid Testing: The Amsler grid is a very simple test that can be done at home to detect worsening of macular degeneration. Using your reading glasses, you simply cover an eye and look at the center of the grid square, looking for any areas of distortion. You then repeat the test for the other eye.
This is very important – you MUST do the test with one eye at a time or you may miss distortion occuring in your non-dominant eye.
If you see a sudden change in your Amsler grid, you should notify Dr. Thayer within 48 hours.
 Ocular Coherence Tomography (OCT): Augmenting the dilated examination of your retina Dr. Thayer will perform, you may be imaged with our OCT. This is painless, quick, and covered by insurance. It is a truly invaluable test in the detection and management of macular degeneration. It is particularly helpful in diagnosing wet AMD in its early stages, when the prognosis with treatment is better.
Ocular Coherence Tomography (OCT): Augmenting the dilated examination of your retina Dr. Thayer will perform, you may be imaged with our OCT. This is painless, quick, and covered by insurance. It is a truly invaluable test in the detection and management of macular degeneration. It is particularly helpful in diagnosing wet AMD in its early stages, when the prognosis with treatment is better.
Treatment for Dry AMD is limited to the preventative measures listed above, frequent Amsler grid monitoring (at least weekly), and regular, dilated eye examinations.
If Dr. Thayer detects the Wet form of AMD, you will be referred to a Retina specialist for further treatment. Treatment of wet AMD involves periodic injections of medication, called anti-VEGF medicine, into the eye. This has the potential to reduce the fluid leakage near your focus area that is the hallmark of wet AMD.
Diabetic Eye Disease
a closer look

No DR

Mild DR

Moderate DR

Severe DR

Proliferate DR
overview
Diabetic retinopathy is a diabetes complication that affects eyes. It results from damage to the blood vessels of the retina. At first, diabetic retinopathy might cause no symptoms or only mild vision problems. But it can lead to blindness.
The condition can develop in anyone who has type 1 or type 2 diabetes. The longer you have diabetes, and the less controlled your blood sugar is, the more likely you are to develop this eye complication.
You might not have symptoms in the early stages of diabetic retinopathy. As the condition progresses, you might develop:
- Spots or dark strings floating in your vision (floaters)
- Blurred vision
- Fluctuating vision
- Dark or empty areas in your vision
- Vision loss
Over time, too much sugar in your blood can lead to the blockage of the tiny blood vessels that nourish the retina, cutting off its blood supply. The eye responds by growing new blood vessels, but these new blood vessels don’t develop properly and can leak easily.
There are two types of diabetic retinopathy:
- Early diabetic retinopathy. In this more common form — called nonproliferative diabetic retinopathy (NPDR) — new blood vessels aren’t growing (proliferating).
- When you have NPDR, the walls of the blood vessels in your retina weaken. Tiny bulges protrude from the walls of the smaller vessels, sometimes leaking fluid and blood into the retina. Larger retinal vessels can begin to dilate and become irregular in diameter as well. NPDR can progress from mild to severe as more blood vessels become blocked.
- Sometimes retinal blood vessel damage leads to a buildup of fluid (edema) in the center portion (macula) of the retina. If macular edema decreases vision, treatment is required to prevent permanent vision loss. This condition is the most common way in which diabetic retinopathy causes vision loss.
- Proliferative diabetic retinopathy (PDR). This is the most severe form of diabetic retinopathy. In this type, damaged blood vessels close off, causing the growth of new, abnormal blood vessels in the retina. These new blood vessels are fragile and can leak into the gel that fills the center of the eye (vitreous).
- Eventually, scar tissue from the growth of new blood vessels can detach the retina from the back of the eye. If the new blood vessels interfere with the normal flow of fluid out of the eye, pressure can build in the eyeball, giving rise to a particularly aggressive type of glaucoma known as Neovascular Glaucoma.
Anyone who has diabetes can develop diabetic retinopathy. The risk of developing the eye condition can increase as a result of:
- Having diabetes for a long time
- Poor control of blood sugar level
- High blood pressure
- High cholesterol
- Pregnancy
- Tobacco use
- Being Black, Hispanic or Native American
You can’t always prevent diabetic retinopathy. However, regular eye exams, good control of your blood sugar and blood pressure, and early intervention for vision problems can help prevent severe vision loss.
Things you can do:
- Manage your diabetes. Make healthy eating and physical activity part of your daily routine. Try to get at least 150 minutes of moderate aerobic activity, such as walking, each week. Take oral diabetes medications or insulin as directed.
- Monitor your blood sugar level. You might need to check and record your blood sugar level several times a day — or more frequently if you’re ill or under stress. Ask your doctor how often you need to test your blood sugar.
- Ask your doctor about a glycosylated hemoglobin test. The glycosylated hemoglobin test, or hemoglobin A1C test, reflects your average blood sugar level for the two- to three-month period before the test. For most people with diabetes, the A1C goal is to be under 7%.
- Keep your blood pressure and cholesterol under control. Eating healthy foods, exercising regularly and losing excess weight can help. Sometimes medication is needed, too.
- Stop smoking.
- Pay attention to vision changes. Contact your eye doctor right away if your vision suddenly changes or becomes blurry, spotty or hazy.
- DO NOT BURY YOUR HEAD IN THE SAND! Ignoring your diabetes, especially in youth, is always a mistake.
Dilated Eye Examination: Dilated eye exams are recommended for all diabetics on an annual basis. Once any degree of diabetes is detected in the eye, these exams should be done more frequently. Dr. Thayer will recommend the frequency of dilated examinations you should have based on the severity of your disease.
 Ocular Coherence Tomography (OCT): If Dr. Thayer detects diabetic signs in your eyes, you may be imaged with our OCT. This is painless, quick, and covered by insurance. It is a very helpful tool in the detection and management of macular edema (swelling).
Ocular Coherence Tomography (OCT): If Dr. Thayer detects diabetic signs in your eyes, you may be imaged with our OCT. This is painless, quick, and covered by insurance. It is a very helpful tool in the detection and management of macular edema (swelling).
In all stages of diabetes, good control of blood pressure and sugar are essential. The early stages of diabetic retinopathy usually do not need any treatment beyond these measures. There are five main complications that require treatment:
- Macular Edema: This swelling in the focus area of the eye is treated with either drops, laser, or injections of medication into the eye. If injections are required, Dr. Thayer will refer you to a local Retina specialty group.
- Vitreous Hemorrhage: This is bleeding within the eye that causes vision filminess or downright vision loss. If Dr. Thayer detects this complication, you will be referred to the Retina group for special imaging to detect the source of the bleeding and to determine the best treatments to avoid further complications.
- Proliferative Diabetic Retinopathy: In this case of abnormal new blood vessel growth in the eye, management options include laser and injections into the eye of a compound that slows new blood vessel growth. These compounds are known as anti-VEGF, or anti Vascular Endothelial Growth Factor. This complication must be dealt with urgently as it can lead to vitreous hemorrhage, retinal detachment, and eye pressure problems.
- Neovascular Glaucoma: This is a particularly aggressive type of glaucoma resulting from abnormal blood vessel formation on the iris and in the drainage angle of the eye. If the drainage angle is blocked by this process, eye pressure can be very difficult to control, leading to blindness. Management includes drops, laser, and intraocular injections of anti-VEGF compounds.
- Traction Retinal Detachment: This is a late stage complication in which abnormal blood vessels or blood within the eye trigger the formation of traction bands that pull the retinal off of its bed. Prognosis is poor here, and management is performed by a Retina surgeon.
Posterior Vitreous Detachment (PVD)
a closer look
A posterior vitreous detachment (PVD) is an universal occurrence as we age. It is commonly known as a floater, and occurs as the vitreous, the gel that fills the back of the eye, undergoes aging changes. In youth, the vitreous is tethered to the optic nerve head and is attached in a 360 degree band around the front part of the retina. As we age, the vitreous gel liquifies and contracts. Eventually, it pulls away from it attachment to the optic nerve, giving one a PVD, or a floater. Up to 15% of the time, a PVD will also cause a retinal tear. Therefore, patients having an acute PVD should undergo a dilated retinal exam without delay. PVD’s can also be associated with macular holes and epiretinal membranes.
Symptoms of a PVD include any or all of the following: “cobweb” or “string-like” floaters, light flashes similar to a strobe going off in the peripheral vision, or a curtain-like shade over the vision.
No treatment is usually necessary or possible for a PVD, unless it is associated with a retinal tear.

